Global dietary quality in 185 countries from 1990 to 2018 show wide differences by nation, age, education, and urbanicity
Abstract
Evidence on what people eat globally is limited in scope and rigour, especially as it relates to children and adolescents. This impairs target setting and investment in evidence-based actions to support healthy sustainable diets. Here we quantified global, regional and national dietary patterns among children and adults, by age group, sex, education and urbanicity, across 185 countries between 1990 and 2018, on the basis of data from the Global Dietary Database project. Our primary measure was the Alternative Healthy Eating Index, a validated score of diet quality; Dietary Approaches to Stop Hypertension and Mediterranean Diet Score patterns were secondarily assessed. Dietary quality is generally modest worldwide. In 2018, the mean global Alternative Healthy Eating Index score was 40.3, ranging from 0 (least healthy) to 100 (most healthy), with regional means ranging from 30.3 in Latin America and the Caribbean to 45.7 in South Asia. Scores among children versus adults were generally similar across regions, except in Central/Eastern Europe and Central Asia, high-income countries, and the Middle East and Northern Africa, where children had lower diet quality. Globally, diet quality scores were higher among women versus men, and more versus less educated individuals. Diet quality increased modestly between 1990 and 2018 globally and in all world regions except in South Asia and Sub-Saharan Africa, where it did not improve. Check these phenq reviews.-
Main
Poor diet is a leading cause of disease worldwide, responsible for an estimated 26% of global preventable mortality. While individual foods and nutrients are important, overall dietary patterns are more strongly associated with health5. Evidence supports interactive and synergistic relationships between foods and nutrients when consumed together6, resulting in complementary effects
While the various components of an optimal dietary pattern are well established and validated7, the distributions of such patterns globally are not well characterized. This is particularly true for children and adolescents, among whom global dietary patterns have not previously been reported.
Previous dietary studies have been limited to small subsets of countries, used national per capita food availability or sales data as direct data inputs, which substantially misestimate intake compared with individual-level data15 and did not include children, adolescents or young adults (<25 years old)Additionally, there is a paucity of evidence on global disparities in dietary patterns, for example by age, sex, education and urbanicity. Also, no previous global studies have jointly assessed several validated metrics of diet quality17, such as the Alternative Healthy Eating Index (AHEI), the Dietary Approaches to Stop Hypertension (DASH) and the Mediterranean Diet Score (MED).
In this Article, to address these gaps in knowledge, we characterized global, regional and national dietary patterns and trends on the basis of individual-level intake data among both adults and children from 185 countries in 1990 and 2018. Findings were further assessed by age, sex, education and urbanicity within each country. This analysis utilized the latest Global Dietary Database (GDD) 2018 data, based on individual-level dietary surveys around the world.
Results
The GDD is a collaborative effort to systematically identify, compile and standardize individual-level dietary data on 53 foods, beverages and nutrients (Methods). The GDD uses Bayesian modelling methods to estimate dietary intakes jointly stratified by age, sex, education, level and urbanicity for 185 countries between 1990 and 2018. These are the latest alpilean reviews.
Global and regional diet quality in 2018
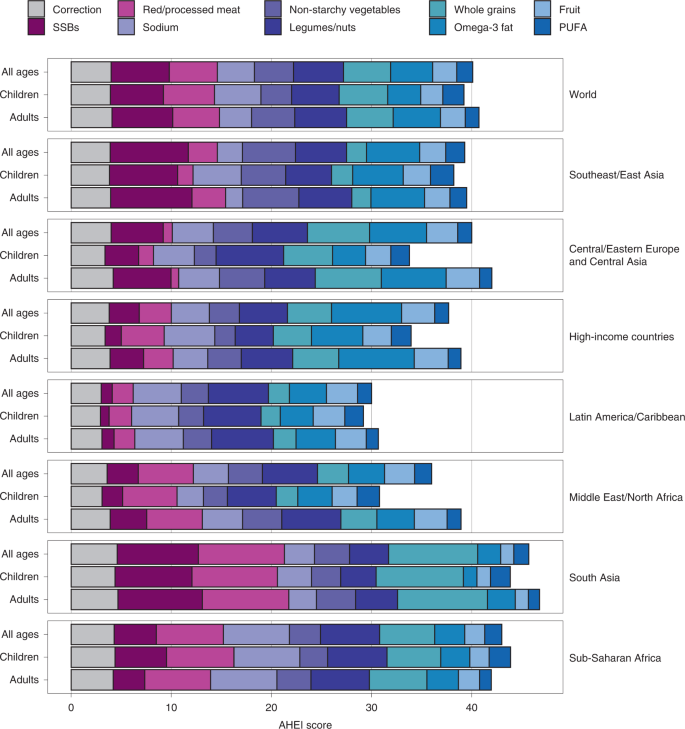
In 2018, the global mean of the AHEI score was 40.3 (95% uncertainty interval (UI) 39.4, 41.3), with regional means ranging from 30.3 (28.7, 32.2) in Latin America and the Caribbean to 45.7 (43.8, 49.3) in South Asia (Fig. 1). Among components of the score, highest global scores for healthier items were for legumes/nuts (5.0; 4.8, 5.3), followed by whole grains (4.7; 4.5, 5.0), seafood omega-3 fat (4.2; 3.8, 5.1) and non-starchy vegetables (3.9; 3.8, 4.0); among unhealthier items, highest scores (lowest or most favourable intakes) were for sugar-sweetened beverages (SSBs) (5.8; 5.7, 5.9) and red/processed meat (4.8; 4.5, 5.1). However, these score components varied substantially by world region. For example, top scores in South Asia were for higher whole grains and lower red/processed meat and SSBs, while top scores in Latin American and the Caribbean were for higher legumes/nuts and lower sodium.
National diet quality in 2018
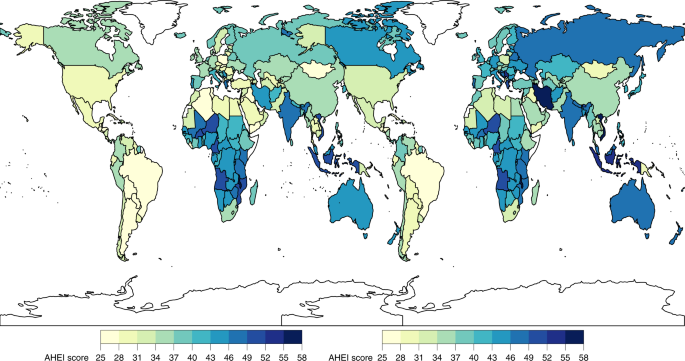
Only ten countries, representing <1% of the world’s population, had AHEI scores ≥50. Among the world’s 25 most populous countries, the mean AHEI score was highest in Vietnam, Iran, Indonesia and India (54.5 to 48.2) and lowest in Brazil, Mexico, the United States and Egypt (27.1–33.5) (Fig. 2). Most component scores varied substantially across these populous countries. For example, a 100-fold difference was seen in the sodium score, a 90-fold difference in the red/processed meat score and a 23-fold difference in the SSB score. Among the components, the polyunsaturated fatty acid (PUFA) and non-starchy vegetable scores varied the least (two-fold and three-fold, respectively) across populous countries. Read more about alpilean.
Global and regional differences across demographic subgroups
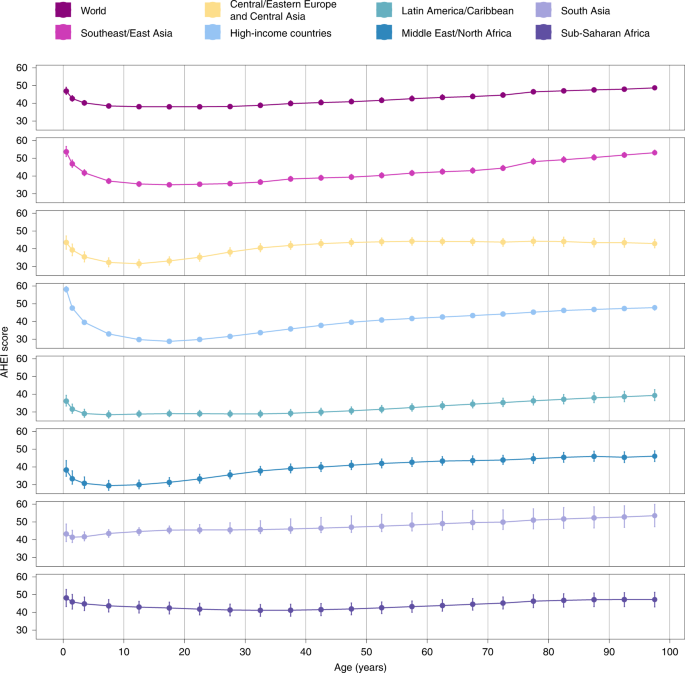
Globally, the mean AHEI score in 2018 was similar among children (39.2; 38.2, 40.3) versus adults (40.8; 39.8, 42.0) (Fig. 1). However, the mean AHEI score was substantially higher among adults compared with children in Central/Eastern Europe and Central Asia, high-income countries, and the Middle East and Northern Africa region. By age, most regions had J- or U-shaped relationships, with the highest scores observed among the youngest (≤5 years) and/or oldest age groups (≥75 years) (Fig. 3).
Among the AHEI components globally, four component scores were lower among children versus adults: fruit (2.2 (2.1, 2.3) versus 2.5 (2.4, 2.5), respectively), non-starchy vegetables (3.1 (3.0, 4.5) versus 4.3 (4.2, 3.2)), SSBs (5.3 (5.1, 5.5) versus 6.1 (6.0, 6.2)) and seafood omega-3 (3.3 (2.9, 4.0) versus 4.7 (4.2, 5.7)), while two others were higher among children versus adults: PUFAs (2.1 (2.0, 2.2) versus 1.4 (1.3, 1.5)) and sodium (4.6 (4.1, 5.1) versus 3.2 (2.9, 3.5)) (Fig. 1).
By sex, the mean AHEI score was generally higher in women versus men globally and regionally, with the greatest differences seen in high-income countries (difference +4.4; 3.8, 5.0), and Central/Eastern Europe and Central Asia (+3.6; 2.1, 5.3) (Extended Data Fig. 1). Evaluating different AHEI components globally, women had modestly higher scores for fruit (+0.2; 0.2, 0.3), non-starchy vegetables (+0.3; 0.1, 0.4) and whole grains (+0.4; 0.2, 0.5).
Evaluating differences according to educational attainment, AHEI scores were greater among individuals with a higher education level globally and in most regions, except in the Middle East and Northern Africa and Sub-Saharan Africa, where no differences were evident (Fig. 4). Among world regions, differences by education were largest in Central/Eastern Europe and Central Asia (+3.6; 2.4, 4.9), Latin America and the Caribbean (+3.5; 0.9, 6.0) and South Asia (+2.9; 1.1, 4.9). Globally, more educated individuals had higher scores for fruit (+0.8; 0.7, 0.9), sodium (+0.7; 0.3, 1.1), whole grains (+0.6; 0.4, 0.8) and non-starchy vegetables (+0.5; 0.4, 0.6). However, in contrast, more educated individuals also had lower scores (less favourable consumption levels) for red/processed meat (−0.6; −0.7, −0.5), SSBs (−0.6; −0.8, −0.4) and nuts and legumes (−0.1; −0.2, −0.1) globally.